
Article begins
Cancerous Heat in the Body
In the embodied experience of a person with cancer, heat plays a critical role.
Hot flashes and night sweats afflict many patients. Sudden-onset surges of intense warmth followed by profuse sweating can be triggered by chemotherapy, radiotherapy (or radiation), hormone therapy, steroid use, or surgery to the reproductive organs that prompt hormonal changes. Both men and women report hot flashes resulting from disease and treatment; in addition, young female patients may also experience hot flashes due to premature, medically induced menopause to protect ovarian reserves from iatrogenic infertility.
But the effects of heat on cancer patients aren’t confined to discomfort. Neutropenic fever, a condition where body temperature rises dangerously high as patients’ white blood cell counts plummet during treatment intervals, is one of the riskiest complications of cancer treatment. Neutrophils are a type of white blood cell that attack bacteria; because chemo and radiation can destroy neutrophils or bone marrow (which produces neutrophils) as a side effect, patients with cancer are often left with immune systems that lack the ammunition to fight everyday bacteria which would otherwise be harmless. Without enough white blood cells, immunosuppressed patients have deficient capacity to jump-start the inflammatory response necessary to fight infection. Therefore, neutropenic fever in a cancer patient is an emergency and can swiftly escalate to life-threating or life-ending illness.
Certain cancers and their treatments also cause peripheral neuropathy, a nerve-damaging side effect that produces a burning sensation in the limbs, hands, and feet. Not only does peripheral neuropathy create a fiery feeling in the extremities, but it also reduces the ability to sense changes in temperature, making those affected vulnerable to burns and injuries. Another side effect known as hand-foot syndrome (palmar-plantar erythrodysesthesia) can cause redness, burning, inflammation, and blistering, resembling a sunburn, on the palms and soles of the feet.
The inability of patients with cancer to thermoregulate (control their body temperatures), the steady risk of becoming febrile, and bodily sensations of burning deeply affect both their comfort and their safety, no matter the climate in which they live. But increasing global temperatures due to the current climate crisis compound the problem, posing further risk of dehydration, heat stroke, and sunburn. Patients who travel to medical appointments and those without access to air-conditioning at home or in hospitals are especially vulnerable.
Cancer and its chemical treatments brings uncomfortable, inevitable, and even dangerous heat.

Cancerous Heat in the World
Not only do smoldering temperatures from the climate crisis worsen conditions for existing cancer patients, but malignant heat also renders well bodies more susceptible to disease. Cancer is already a major public health problem, with over 19 million incident cases and nearly 10 million deaths globally in 2020, and higher rates of cancer (especially lung, skin, and gastrointestinal) are projected to accompany extreme global temperatures.
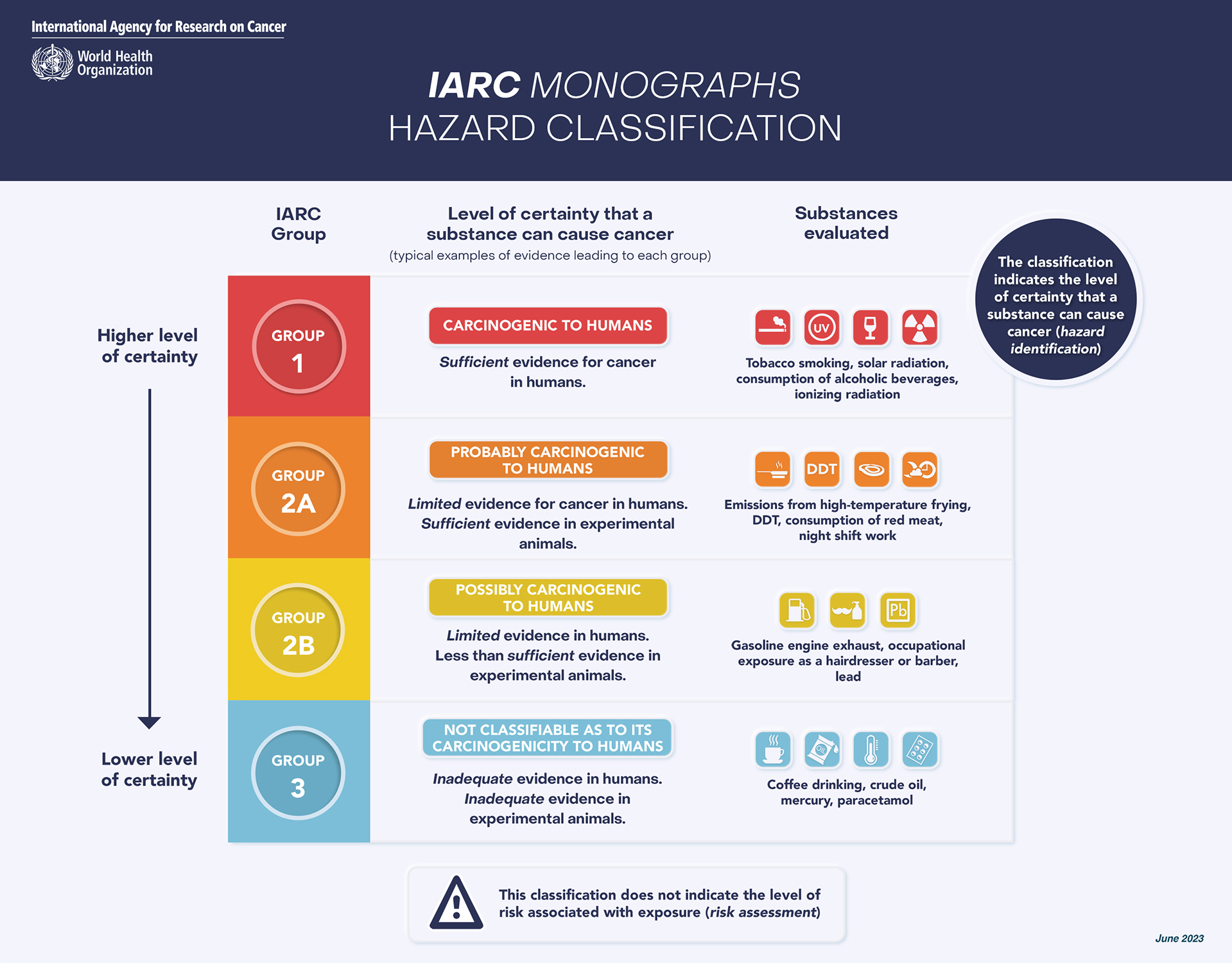
Outdoor pollution (arising, in part, from burning fossil fuels, coal-fired power plants, oil and gas extraction, and fracking) was classified in 2015 by the International Agency for Research on Cancer as a group 1 carcinogen, meaning sufficient evidence exists to conclude that hazardous ambient air particle matter causes cancer in humans. Several other cancers, such as head and neck, oral, liver, bladder, and kidney cancers, have been shown to be associated with polluted air exposure as well. Particle matter resulting from destabilized, overheated natural sources—such as dust, volcanoes, sea spray, and wildfires—also contributes to new cancer diagnoses. An estimated 410 megatons of carbon were released into the atmosphere in 2023 by Canadian wildfires alone; record-breaking wildfires sweeping boreal forests in recent years exposed those residing within 50 km of the fires to carcinogen soot, as well as contributed to greenhouse gas emissions globally.
{kind=link}
Prolonged exposure to ultraviolet (UV) radiation from the sun’s rays is also a major risk factor for melanoma (skin cancer). The depletion of the ozone layer from greenhouse gas effects intensifies the potency of ambient UV and accelerates the dangers of exposure. Furthermore, regions that have been historically limited in their sun exposure during the cold winter months have now warmed, and those living in these changing climates spend more time outside throughout the year. While many high-income countries have implemented prevention efforts against malignant melanoma, such as educational campaigns like the World Health Organization’s INTERSUN program initiative, individuals living in low- and middle-income nations, especially near the equator or in higher altitudes, remain at increased risk for UV damage. These nations also usually have less medical infrastructure to detect and treat skin cancer.
Gastrointestinal cancers resulting from consuming polluted food and water are also emerging alongside warming climates. As the surface temperature of Earth rises and increased humidity causes excessive rainfall and flooding, the risk of carcinogenic pollutants passing into irrigation and agriculture systems has become a steady threat. After Hurricane Harvey hit the Gulf Coast of Texas in 2017, for example, more than 500 industrial chemical plants, oil refineries, and hazardous waste sites were flooded, and carcinogenic toxins were circulated among residential and commercial irrigation infrastructures throughout the Houston region.
Worsening air quality, broadened UV radiation exposure, and higher rates of environmental toxins are all ways in which the heat of our world is already impacting cancer rates, as well as the comfort and safety of cancer patients.
Metastatic Supply Chains
While scorching global temperatures produce downstream effects that cause higher rates of cancer, healthcare and treatment options for people with cancer are also structurally vulnerable to climate-related disturbances.
Extreme weather events cause power outages that threaten or derail clinic and laboratory operations, medical equipment use and production, and communication systems—not to mention patient transportation—which negatively impact the availability and effectiveness of the infrastructure patients depend on for diagnosis and treatment. Major weather events and the subsequently destabilized or depressed economies in the areas they affect may drive specialized healthcare personnel away, while the residents left behind are already vulnerable and sometimes unable to travel for treatment. Patients with fast-growing cancers are especially disadvantaged, since adherence to a s